People living in redlined neighborhoods in 1940 didn’t live as long as those living in neighborhoods with access to credit and home loans, according to a new paper by researchers at the University at Buffalo and Texas A&M University.
That disparity continues today.
The study, “Individual-Level Exposure to Residential Redlining in 1940 and Mortality Risk,” was published in September in JAMA Internal Medicine. The journal also published an editorial highlighting the findings.
Legalized racial discrimination
“Redlining is an example of structural racism because it put into law a policy that fostered discrimination based on race,” says Leonard E. Egede, MD, Charles and Mary Bauer Endowed Chair of Medicine in the Jacobs School of Medicine and Biomedical Sciences at UB, who co-authored the paper with Sebastian Linde, Ph.D., of Texas A&M University School of Public Health. Egede is also president of UBMD Internal Medicine of UBMD Physicians’ Group.
Redlining originated with the Home Owners Loan Corporation (HOLC), which was created in 1933 as part of the New Deal.
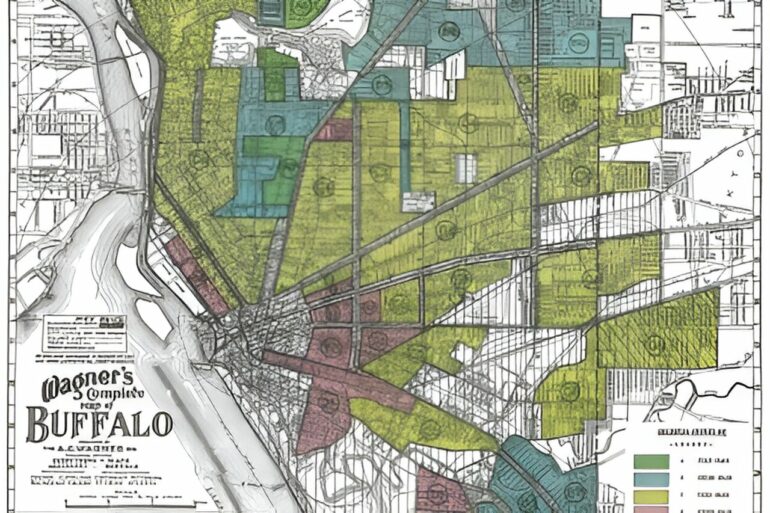
HOLC ranked the supposed “creditworthiness” of neighborhoods in American cities by designating each neighborhood with a color: Green was the most creditworthy, blue was still desirable, yellow indicated decline and red was the worst. Redlined neighborhoods were home to racial and ethnic minorities, primarily African Americans.
The researchers linked individuals living in HOLC-ranked neighborhoods in 1940 with death records from age at death from the Social Security Numident file. They found that each grade drop from one color to the next was associated with an 8% increased risk of death later in life, a decline in life expectancy of .49 years. Compared to people living in neighborhoods deemed the best credit risks—primarily white neighborhoods—those living in redlined neighborhoods had a life expectancy gap at age 65 estimated at being 1.47 years shorter.
The study used information from the Mapping Inequality project, which has a map of cities that were redlined.
When people think about redlining and residential segregation, Egede says, they typically think of major cities like New York City and Chicago, but he notes that HOLC maps were completed for 239 cities across the U.S.
In Western New York, for example, HOLC maps were created for Buffalo, Niagara Falls, Rochester, Jamestown and Elmira.
Long after they were outlawed, the effects of the HOLC maps persist.
“HOLC maps can be conceptualized as reflections of historical beliefs about race, place and value,” Egede says, beliefs that, he adds, are often replicated in the planning and development of suburban areas.
“Although the Fair Housing Act of 1968 prohibited redlining, several studies have identified associations between neighborhood-level exposure to historic redlining and present-day neighborhood-level health and mortality outcomes,” explains Egede. “Premature and excess mortality in any group is unfair and can carry many hidden losses, such as entire communities not benefiting fully from age-related entitlements such as Social Security and Medicare.”
A loss of more than $20 million per 1,000 residents
One way to calculate those losses over the long term, Egede says, would be to compare the amount of Medicare benefits that individuals in redlined neighborhoods received compared to the amount that those living in the “best” (i.e., coded green) neighborhoods received. He says that with their reduced life expectancy, from 1940 to 2005, 1,000 residents in the redlined neighborhoods would utilize approximately $22.6 million less than would 1,000 residents in the “best” neighborhoods.
“Therefore, not only are individuals not benefiting fully from age-related entitlements provided by the federal government, but neighborhoods are not receiving the benefits of the longer lives of their residents,” Egede says.
Redlining also created a “dual housing market,” explains Egede. “African Americans were subject to different procedures when purchasing a home than white Americans,” he says.
This has had the effect of restricting the flow of capital into and out of minority neighborhoods, making it much more difficult or impossible to purchase homes and businesses, and build wealth. These challenges also lead to social risk factors, lower human capital and lower health care resources, all of which have been linked to adverse health outcomes and premature mortality.
Buffalo is an example
“Buffalo is an example of this, unfortunately,” Egede observes, noting that the Buffalo-Niagara metro area is ranked within the top 10 most segregated in the nation.
“The segregation by neighborhood that happened in the 1940s and 1950s is playing out into the 2010s and 2020s,” he says. “Eighty-five percent of African Americans within the city of Buffalo live east of Main Street, and there are known disparities in life expectancy today for individuals east of Main Street compared to west of Main Street, and between whites and African Americans within the city.”

He adds that as recently as 2014 a Buffalo bank was charged with redlining by the state attorney general, having created a map that defined the area in which they would market their services, excluding the East Side of Buffalo. From 2009 to 2012, less than 1% of the residential mortgages at this bank went to African American borrowers.
In the editorial accompanying the paper, Mary T. Bassett, MD, of Harvard University illustrates how neighborhoods that were historically redlined are still compromised today, experiencing disparities in all sectors and contributing to a broad range of adverse health outcomes for residents of all ages.
“Many people think that once a law is changed the impact of that law is removed,” Egede says. “However, that is not what we are seeing with historical redlining.”
Egede and his colleagues are currently studying how to reduce the impacts of structural racism on health disparities.
More information:
Sebastian Linde et al, Individual-Level Exposure to Residential Redlining in 1940 and Mortality Risk, JAMA Internal Medicine (2024). DOI: 10.1001/jamainternmed.2024.4998
Mary T. Bassett, Racial Residential Segregation, Redlining, and Health, JAMA Internal Medicine (2024). DOI: 10.1001/jamainternmed.2024.5011
Provided by
University at Buffalo
Citation:
Living in a redlined neighborhood in 1940 was a risk factor for premature death, and the disparity persists today (2024, October 10)

