
Black women at high risk of breast cancer face a variety of obstacles that may keep them from care that could prevent cancer and increase the chances they’ll survive if they develop the disease, new research has found.
A study from researchers at The Ohio State University provides insights into the factors that contribute to racial disparities in use of preventive measures, including genetic testing, prophylactic mastectomies and medication to thwart breast cancer.
In the new study, which appears today (March 1, 2023) in the journal PLoS ONE, the researchers interviewed 20 Black women and 30 white women at high risk of breast cancer to better understand racial differences in the decision-making process, which hadn’t previously been well-studied.
Among their findings: Black women may be less focused on breast cancer risk as an issue to be addressed proactively, may less frequently possess information to help guide their decisions about prevention, and face more constraints when it comes to making and carrying out health-protective decisions.
“We need to recognize that the personal, interpersonal and social dynamics that Black women are experiencing that influence their ability to cope with their risk are complicated and multilayered and need to be taken into account if we’re going to empower people to do something about their risk,” said Tasleem Padamsee, lead author of the study and an assistant professor in Ohio State’s College of Public Health.
Women with strong family histories of breast cancer, genetic predispositions to the disease or other risk factors can face a 20% to 80% risk of developing the disease within their lifetimes, but can cut that risk in half, or more, by using preventive therapies, research has shown. Black women in the U.S. are diagnosed with breast cancer at about the same rate as white women, although at younger ages and later stages of disease, and with higher breast cancer mortality rates.
“I walked away from these conversations feeling like many of these women have experienced horrible things with cancer over and over again, and that they just have an overriding sense that cancer is this thing that comes at you, upends your life and the life of everyone around you, and it’s up to God what happens from there,” said Padamsee, who is a member of The Ohio State University Comprehensive Cancer Center’s Cancer Control Research Program.
“Being in a cutting-edge cancer center, we have ways, and are finding new ones, to head the disease off at the pass and—if we can’t—to catch it earlier, when the prognosis is much better. And we want all high-risk women to have those advantages.”
The researchers found several differences based on race, all of which pointed to potentially worse outcomes for the high-risk Black women.
Overall, the Black women in the study described feeling less ready and equipped to consider and cope with their risk and less informed about their options. They also reported facing more obstacles in availing themselves of those options and having less access to detailed information to help them make decisions about managing their risk.
Previous research using data from the same interviews with this group of women found that experiences with family members had a profound influence on perceptions of their own risk and prevention options. Though Black women generally reported having more up-close experiences with family members who had cancer, that didn’t seem to be associated with awareness of measures they might take to protect themselves, Padamsee said.
The Black women in the study were more likely to describe cancers as a collective group of diseases for which they have an equally high risk, rather than recognizing a particular predisposition to breast cancer. Women who thought this way did not generally believe anything specific could be done to prevent their increased risk, instead viewing a healthy lifestyle and regular health screenings as their sole tools to mitigate risk.
Many white women in the study who were more inclined to pursue preventive medication, such as Tamoxifen, or prophylactic mastectomies, told the researchers they perceived themselves to be at specific risk of breast cancer and that they worried a lot about its impact on them and their families.
In contrast, Black women in the study who worried about their cancer risk were more likely to talk about their faith.
“We’re just a really spiritual family, we believe in God. … I put my faith in God in that everything will be alright,” said one of the middle-aged Black women interviewed for the study.
While worrying less and having a stronger spiritual connection could have mental health benefits for Black women, it also could serve as a barrier to seeking out risk-management options, Padamsee said.
Black women in the study were also more likely to describe other priorities in their lives—including family and work demands and other health struggles—that were top of mind. About 20% of white women in the study had a major health concern besides the high risk of breast cancer, compared to 40% of the Black women.
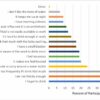
Access to care from specialists, including genetic counselors, was also uneven. About 15% of the Black women reported access to specialists, compared to 70% of the white women.
That disparity likely has a significant influence on another key finding—that Black women were less likely to know about preventive measures and were much less likely to undergo genetic testing even when they’d heard of it.
Black women’s ability to manage their breast cancer risk also is more significantly impacted by financial barriers, the study suggests. Of the Black women in the study, 40% had experienced a time without insurance, compared to just 3% of the white women. And 40% of the Black women also described significant financial difficulties coping with health challenges, compared to 3% of whites.
These new findings could provide a foundation for building equity within health care, Padamsee said. Among the possibilities she suggests: Find better ways to acknowledge and incorporate patients’ spirituality and religious perspectives into discussions about prevention, ensure that women have access to good insurance coverage or other ways of paying for specialist care, and improve training for primary care physicians who are often the sole source of medical counsel for high-risk Black women.
“There’s a lot of hand waving when it comes to talking about health equity problems, and discrimination and disadvantage in general,” she said. “One of the things that’s really important in equity work is that we have clear documentation of where the differences are and where they’re coming from, and this study helps provide that.”
Provided by
The Ohio State University
Citation:
Obstacles for breast cancer prevention in high-risk Black women (2023, March 1)

