Location, race and insurance status play a significant part in the odds of a patient being diagnosed with early-stage or late-stage cancer, according to a detailed medical records analysis of more than 94,000 patients with cancer by researchers at the Johns Hopkins Bloomberg School of Public Health and the Johns Hopkins Kimmel Cancer Center.
Patients who lived farther away from a facility designated a comprehensive cancer center (CCC) by the National Cancer Institute (NCI) and who received only a diagnosis or only treatment at the center had higher than average odds of a late-stage diagnosis, as did non-Hispanic Black patients and patients with Medicaid or no insurance, regardless of their location, the researchers report.
The work, published in JAMA Network Open, highlights that significant barriers to cancer screening and treatment remain to be addressed for people living far from a CCC and for disadvantaged populations.
Previous studies showed that patients who do not receive their first treatment at a CCC experience worse cancer outcomes. Investigators including Michael Desjardins, Ph.D., an assistant research professor of epidemiology and a core faculty member at the Spatial Science for Public Health Center at the Bloomberg School of Public Health; Frank Curriero, Ph.D., professor of epidemiology and director of the Spatial Science for Public Health Center; and William Nelson, M.D., Ph.D., director of the Kimmel Cancer Center, initiated an exploratory study to determine how proximity to a CCC and other social determinants of health affect the odds of receiving a diagnosis of an early-stage or late-stage cancer.
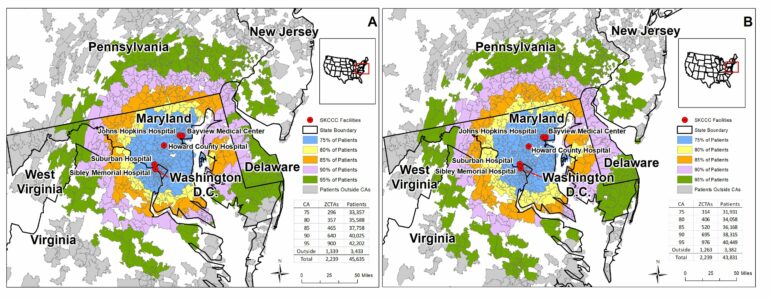
First, the team tackled how to define the region, or “catchment area,” served by a CCC. There is no standardized approach to defining a catchment area among the 54 NCI-designated CCCs nationally. Some centers identify nearby counties with the highest proportion of their patients with cancer, others define areas based on ratio of cancer cases compared to all cancer deaths, and centers use many additional methods.
Desjardins, who specializes in geographic information science and health, developed a simple yet intuitive approach to define and evaluate a catchment area: Focus on the closest 75% of patients as determined by miles along the road network using a geographic mean center of Johns Hopkins’s five hospitals.
The team analyzed health and demographic data from 94,007 patients in the Johns Hopkins Hospital cancer registry who had received a cancer diagnosis, cancer treatment, or both a diagnosis and treatment from 2010 to 2019. Significant disparities in cancer staging quickly emerged.
Non-Hispanic Black patients had higher odds of receiving a late-stage cancer diagnosis compared to average, even if they lived close to the Kimmel Cancer Center. That finding aligns with a body of work that finds lower odds of cancer survival for non-Hispanic Black patients, and it suggests that accessibility to health care is more complex than geographic distance alone.
Also, people with no insurance, unknown insurance or Medicaid also had higher odds of receiving a late-stage cancer diagnosis. This finding underscores the challenge that people with low income face in accessing health care, especially for cancer treatment.
Finally, patients who lived outside the 75% catchment area and received only treatment or only a diagnosis at a CCC also had higher odds of a late-stage diagnosis. While travel distance could be a factor in seeking only a diagnosis or only treatment, the finding suggests that some CCC patients rely on more than one facility for their cancer care.
“Moving forward, we need to ask patients why they choose a particular cancer center for a diagnosis or a treatment,” says Desjardins. “Maybe they can’t afford the treatment at a certain location, or maybe they are seeking a specific late-stage cancer treatment. There are a lot of nuances we have to try to understand by combining spatial data sets with qualitative surveys.”
“NCI-designated cancer centers are committed to improving cancer care and outcomes throughout their catchment areas, particularly to communities and populations that have been historically underserved,” Nelson adds. “To do so, they will need to work with partners, embracing new technologies and tactics.”
The study authors say diagnosis and treatment ideally should both occur at a CCC, if possible — people diagnosed and treated at a CCC had the lowest odds of a late-stage diagnosis.
Additionally, CCCs across the country can and should adopt a standardized approach to assessing catchment areas, says Desjardins. Then, where areas overlap, centers can communicate with one another to share patient care information.
Additional study co-authors are Norma Kanarek and Jamie Bachman, both of Johns Hopkins.
More information:
Michael R. Desjardins et al, Disparities in Cancer Stage Outcomes by Catchment Areas for a Comprehensive Cancer Center, JAMA Network Open (2024). DOI: 10.1001/jamanetworkopen.2024.9474
Provided by
Johns Hopkins University School of Medicine
Citation:
Proximity to a cancer center contributes to cancer stage at diagnosis, study finds (2024, May 22)

