When I work shifts in the emergency department, I often find myself weighing two imperfect options for patients who might have a sexually transmitted infection. Should I administer antibiotics “just in case,” or wait for lab results to process a day or two later and risk the patient not returning for antibiotics? Based on national guidelines, the ED tends to swing toward coverage.
In our new systematic review published in Academic Emergency Medicine, we find that 38% of ED patients who ultimately test negative for chlamydia or gonorrhea still received antibiotics. While this doesn’t account for patients who may have had infections but were undetected at the time of lab testing, it is still a concerningly high proportion. That is nearly four potentially unnecessary treatments for every 10 patients, contributing to resistance, avoidable side effects and medical costs with questionable clinical benefit.
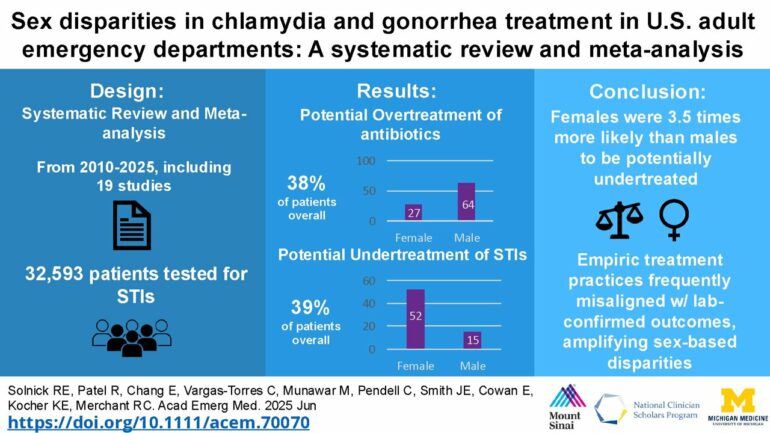
Yet overtreatment is only half the picture. When we pooled 19 U.S. studies spanning more than 32,000 adult ED visits, we discovered another imbalance hiding in plain sight: Women leave undertreated for STIs far more often than men, while men receive antibiotics they may have never needed. The numbers are hard to ignore—and they demand that we rethink how the ED diagnoses and treats two of the most common bacterial STIs in America.
Why are emergency departments critical to STI care?
Chlamydia and gonorrhea are curable bacterial infections, yet they still affect 2.4 million Americans each year. Untreated, they can lead to pelvic inflammatory disease, infertility and chronic pelvic pain—consequences that disproportionately affect women. With STI clinics closing and primary care access strained, EDs increasingly serve as the default setting for STI diagnosis and treatment. These are high-stakes moments. When patients leave the ED, they may not return. That means every treatment decision—whether to give antibiotics now or wait for lab confirmation—matters.
What we found when we looked across 32,000 ED visits
Across the studies in our review, 1 in 7 adults tested for chlamydia or gonorrhea turned out to be positive. Infection rates were higher among men than women—about 25% versus 11%. Almost half of patients received antibiotics before results came back, a practice known as empiric treatment.
But digging deeper revealed a troubling mismatch. Among those who eventually tested negative, 38% had already received antibiotics they may not have needed. Meanwhile, 39% of those who tested positive had no record of receiving appropriate treatment—either during the ED visit or, in some studies, during the follow-up period.
These discrepancies weren’t random. Women were 3.5 times more likely than men to go potentially undertreated, with more than half of all positive cases in women lacking documented treatment. In contrast, men were more than twice as likely as women to be overtreated—antibiotics given even though tests came back negative.
How does this happen?
Several factors contribute. Men, particularly those who are gay or bisexual, can present with clear symptoms and have higher infection rates, prompting clinicians to treat on the spot. Women, on the other hand, are frequently tested as part of a broader evaluation for abdominal or pelvic complaints, many of which turn out not to be STIs. With lower pre-test probability, clinicians may opt to defer treatment until results return.
. Proportion refers to (untreated patients with laboratory-confirmed positive results)/(all patients laboratory-confirmed positive). ES (95% CI) refers to pooled estimates of the proportion (95% CI). GC/CT, gonorrhea/chlamydia. © Rachel E Solnick")
Proportion of ED patients with laboratory-confirmed GC/CT without empiric treatment (potential undertreatment). Proportion refers to (untreated patients with laboratory-confirmed positive results)/(all patients laboratory-confirmed positive). ES (95% CI) refers to pooled estimates of the proportion (95% CI). GC/CT, gonorrhea/chlamydia. © Rachel E Solnick
But bias may play a role, too. Decades of research show that women are often treated less aggressively than men for a wide range of conditions—chest pain, pain control, and now, it seems, STIs. When clinicians may assume lower risk based on sex, this approach increases the chances that a true infection in a woman may go untreated.
What can be done to fix this?
One obvious solution is to bring the lab to the bedside. Rapid molecular tests now exist that can detect chlamydia and gonorrhea in under an hour. In pilot studies, these tests have allowed EDs to make more informed, real-time decisions. If the result is positive, the patient can be treated immediately; if negative, unnecessary antibiotics can be avoided.
Another approach is shared decision-making. For patients at low to moderate risk who are able to follow up, a brief discussion outlining the pros and cons of immediate versus delayed treatment can support more personalized care, and potentially reduce overtreatment.
ED callbacks, which are already common for relaying positive STI results, offer another opportunity. These follow-up calls are a chance not just to provide treatment, but also to offer expedited partner therapy and even start HIV prevention through post-exposure prophylaxis or pre-exposure prophylaxis, when appropriate.
Finally, we can’t fix what we don’t measure. Recognizing and tracking disparities is a crucial first step. Next, integrating clinical decision support into electronic health records—simple prompts that encourage reevaluation of treatment decisions in specific contexts—could help close the gender gap in STI care.

A way forward
The ED is often the main place where some patients will receive STI testing or treatment. But it’s also a setting where quick decisions, made with limited information, can unintentionally reinforce disparities. With better diagnostic tools, thoughtful workflows, and an intentional focus on equity, we can deliver care that’s not just fast but also fair and evidence-based.
Until then, every shift is a reminder that behind these numbers are real people. I imagine having a young woman as a patient, and the chances that she might leave the ED without antibiotics and return months later with pelvic inflammatory disease, or a man who suffers from gastrointestinal side effects from treatment he never truly needed. While we can’t eliminate all diagnostic uncertainty, we can reduce avoidable harm by recognizing patterns, evaluating clinical data, and adjusting our approach based on evidence.
This story is part of Science X Dialog, where researchers can report findings from their published research articles. Visit this page for information about Science X Dialog and how to participate.
More information:
Rachel E. Solnick et al, Sex disparities in chlamydia and gonorrhea treatment in U.S. adult emergency departments: A systematic review and meta‐analysis, Academic Emergency Medicine (2025). DOI: 10.1111/acem.70070
Rachel Solnick, MD, MSc, is an Assistant Professor of Emergency Medicine at the Icahn School of Medicine at Mount Sinai. Her research focuses on HIV prevention, STI care, and maternal health, with an emphasis on expanding access to high-quality reproductive and sexual health care for all emergency department patients. She is the PI of an NIH Career Development Award studying the implementation of HIV pre-exposure prophylaxis (PrEP) for ED patients diagnosed with STIs during telephone callbacks.
Citation:
The hidden problem in emergency department STI care: Overtreating men, undertreating women (2025, June 26)

